Lipid Therapy
Basic Facts
- The aim of lipid therapy is to decrease the risk of heart disease by lowering harmful cholesterol levels.
- Physicians often recommend that patients make lifestyle changes, such as eating a diet lower in fat, exercising, and losing weight.
- If lifestyle changes alone do not lower cholesterol levels enough, the physician may recommend medications.
Lipid is the scientific term for fats in the blood, and the term is used to describe fatty acids, neutral fats, waxes, and steroids. The two main types of lipids that affect heart disease are fatty acids, which can combine to form fats called triglycerides, and cholesterol.
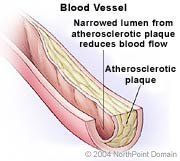
As people age, their coronary arteries may be affected by atherosclerosis, or hardening of the arteries. Atherosclerosis is the buildup of fatty streaks and cholesterol-laden plaque in the walls of the arteries. Abnormal levels of triglycerides and cholesterol in the blood can accelerate atherosclerosis and increase a person's risk of developing heart disease. Coronary heart disease, or CHD, is diagnosed when the accumulation of plaque in a coronary artery grows large enough to obstruct blood flow to the heart muscle.
The body uses a kind of protein called apoprotein to carry the lipids through the blood and into the cells. A lipid bound with a protein is called a lipoprotein, and lipoproteins are classified by their density. The lipoproteins that carry cholesterol are low-density lipoprotein, or LDL, and high-density lipoprotein, or HDL.
Both LDL and HDL carry cholesterol, but because LDL deposits the cholesterol in the body's tissues where it can contribute to problems such as atherosclerosis, it is often called 'bad' cholesterol. HDL, which removes cholesterol from the body, is referred to as 'good' cholesterol. The amount of all the cholesterol carried by both HDL and LDL in the bloodstream is referred to as total cholesterol.
Abnormal levels of total cholesterol, HDL cholesterol or LDL cholesterol, triglycerides are called lipid disorders. One of the most common lipid disorders is hypercholesterolemia, or high cholesterol.
According to the National Cholesterol Education Program, a person with a total blood cholesterol level of 240 milligrams per deciliter, or mg/dL, has twice the heart attack risk of a person with a level of 200 mg/dL, all other factors being equal. A person with a total cholesterol level of 300 mg/dL is 5 times more likely to have a heart attack than a person with a cholesterol level of 200 mg/dL. Reducing total cholesterol can reduce the risk of serious heart problems drastically. For example, 25 percent drop in blood cholesterol levels halves heart attack risk.
Before beginning lipid therapy, physicians establish baseline lipid levels and assess a person's risk of heart disease. A baseline lipoprotein profile is determined from a blood test.
Lowering raised LDL cholesterol levels is the primary target of lipid therapy.
WHAT TO EXPECT
When LDL levels are high enough to add to the risk for CHD, physicians usually recommend people first make changes in their diet and exercise habits.
A major part of a lifestyle change is changing one's diet. For example, physicians recommend that people with lipid disorders receive less than 7 percent of all daily calories from saturated fat, with total fat intake accounting for between 25 and 35 percent of calories each day. Cholesterol intake should be limited to less than 200 mg per day. Other recommendations include increased intake of the soluble fiber found in oats, peas, beans, and certain fruits to between 20 and 30 g each day. An increased intake of plant stanols or sterols, substances found in nuts, some vegetable oils, corn, and rice, can also help reduce LDL levels.
Other foods that help control cholesterol include:
- Cold-water fish;
- Soy; and
- Psyllium (a source of soluble fiber).
Smokers need to quit immediately after finding out they have a lipid disorder. Losing weight can also decrease LDL levels. Increased physical activity is another component of lifestyle changes, but because each person's health condition and tolerance for exercise is different, no set amount of exercise is certain to affect cholesterol levels.
If lipid levels do not improve after 3 months of lifestyle changes, or if a person has CHD or blood lipid levels that are thought to be genetically determined, physicians may consider adding medical therapy to lifestyle changes. Some of the medications used include:
- Statins, which lower levels of LDL and triglycerides by blocking the liver from manufacturing cholesterol;
- Bile acid sequestrants, which block resorption so that LDL levels decrease;
- Fibrates, which have been shown to lower cholesterol and triglycerides in the blood; and
- Niacin, or vitamin B5, which, appears to reduce the breakdown of triglycerides in the liver, in turn preventing fat storage and decreasing LDL.
Although lowering LDL levels remains the primary goal of lipid therapy, other lipid abnormalities may also require treatment.
Low HDL levels. To treat isolated low HDL, niacin or fibrates may be prescribed.
Dyslipidemic syndrome. Treatment of this metabolic syndrome usually involves treating underlying causes, such as weight problems and physical inactivity. Physicians typically recommend lifestyle changes such as weight loss and increased physical activity. When lipid levels remain abnormal despite lifestyle therapies, physicians may prescribe antihypertensive therapy to treat high blood pressure, prescribe aspirin for people with CHD to reduce the formation of clots that may cause angina or heart attack, and treat elevated triglycerides and low HDL levels with medical therapies.
Elevated triglycerides. As with other lipid disorders, the primary objective of therapy in people with elevated triglyceride levels is to reach a set LDL goal. If after reaching an LDL goal a person's triglyceride level remains more than 150 mg/dL, physicians may recommend people intensify their weight management efforts and increase their physical activity.
For people with a triglyceride level between 200 and 499 mg/dL after the LDL goal is reached, physicians may consider adding drug therapy, which might include increasing dosage with an LDL-lowering drug, or adding niacin or fibrate.
If a person's triglyceride level exceeds 500 mg/dL, it must be lowered to prevent pancreatitis, which is an infection or inflammation of the pancreas. Physicians may then prescribe a diet that is very low in fat, with fewer than 15 percent of calories coming from fat. Weight loss and physical activity along with niacin or fibrate therapy may also be recommended.
Copyright © 2017 NorthPoint Domain, Inc. All rights reserved.
This material cannot be reproduced in digital or printed form without the express consent of NorthPoint Domain, Inc. Unauthorized copying or distribution of NorthPoint Domain's Content is an infringement of the copyright holder's rights.